- Vital Shift
- Posts
- Creatine: When a Supplement Works So Well, It Looks Like a Problem
Creatine: When a Supplement Works So Well, It Looks Like a Problem
Issue #26 · Read Time: 4 minutes
Tahsin Khan
March 22, 2026
Creatine doesn’t scare people because of what it does. It scares people because of what they’ve heard. Half-remembered cautions get falsely promoted to unwarranted fears, and once a label sticks, nobody checks the source. This piece peels off the old mythsa and swaps gossip for evidence so your choices rest on solid ground.
What Needs to Shift?
Creatine has been dissected in more studies than any other supplement, yet one rumor won’t die: kidney damage. The cruel twist is that it’s one of the few supplements that delivers, and it can make healthy lab results masquerade as disease.
So, it gets tossed onto the be‑careful pile with other rituals that look like prudence.
A headline, a parent’s warning, a friend’s “kidneys, man,” and suddenly it lives in the “why invite trouble?” category, filed away as a potential danger. The trouble is that this caution isn’t rooted in what’s happening in the body. It’s a hand‑me‑down myth born out of a lack of understanding.
Let’s clear that up with a quick map of creatine’s route, how it involves the kidneys, and why routine testing can potentially steer you wrong.
Behind the Scenes of Creatine’s Journey
Creatine is a natural compound made by the body from amino acids. It helps quickly restore energy (ATP) in muscle cells during intense exercise.
Your body (liver, kidneys, and pancreas) naturally makes about half of the creatine it needs every day; red meat, seafood, and supplementation cover the rest. Once creatine is in the body, three things matter:
Storage: 95% of creatine is stored in muscle. ~5% in the brain.
Breakdown: A small portion of creatine breaks down into creatinine at a constant daily rate. Creatinine is the spent form that has little function. Your body just needs to get rid of it.
Filtration: Creatinine circulates in the blood and your kidneys filter it into urine.
The fuller the creatine tank, the more creatinine you’ll make—think big muscles, heavy meat intake, or supplementation.
↦ Trail through the body: Creatine → Creatinine → Bloodstream → Kidneys → Urine
So, blood creatinine at any given moment reflects two forces:
Make: muscle mass, meat intake, creatine pool size (including supplementation)
Clear: kidney filtration status, hydration status
For most people, the make side barely moves day to day. So when blood creatinine rises, the clear side (kidneys) get the blame.
Why This Matters for Lab Work
Doctors use blood creatinine as a proxy for kidney function.
The logic: because the make side is almost always stable, a rise in blood creatinine often means that the kidneys aren't clearing it well enough. That assumption is baked into the test.
But creatine supplementation breaks the assumption. You've increased the make side. Blood creatinine goes up, not because filtration slowed down, but because you're producing more of it. The test can't tell the difference.
On paper, this misleads individuals into thinking creatine "deteriorates" kidney function.
More sawdust doesn’t mean the shop vac is broken; it might just mean you’re cutting more wood.
⚠️ Fix the Signal: to circumvent this noise, clinicians can utilize Cystatin C—a blood marker that tracks kidney function without being skewed by the body's creatine levels or muscle mass.
Does Creatine Damage Healthy Kidneys?
No.
Five-year follow-ups across hundreds of studies over three decades found no harm to kidney function in healthy individuals. See Appendix A.
⚠️ Exception: if pre-existing kidney disease is already present, the calculus changes. Creatine supplementation in this population should be approached with a dose of oversight and caution. Talk to your doctor if this is you.
The concerns beyond kidneys are minor: dose‑related gastrointestinal upset and minor reversible water weight, with no blood pressure or liver concerns. See Appendix B.
The Hair Scare
If creatine has a boogeyman, it’s hair loss in men. I like my waves; they’re one of the few freebies I got from genetics, and I’m not donating them to folklore. With my hairline on the line, I’m going to comb through the data strand by strand.
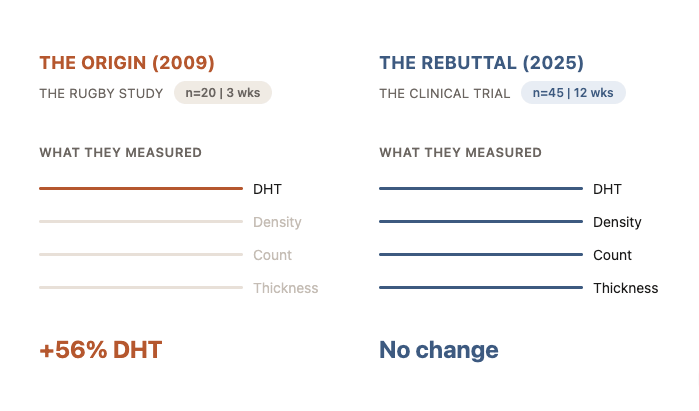
Origin of the Myth (2009): One small study of 20 rugby players saw DHT jump 56% after a brief creatine loading phase. Because DHT drives male‑pattern baldness, the street-level takeaway turned into: creatine = ↑ DHT = ↑ hair loss. [1]
The Critique: Three cracks weaken the study’s argument.
Skewed starting point: the creatine group began with abnormally low DHT, so the “increase” mostly shows them climbing back toward normal, not a pathological spike.
No hair outcomes: the study never measured hair follicles, hair density, or any hair for that matter; just DHT.
Failure to replicate: in the 15 years since, no other study managed to reproduce the result.
Long-Awaited Rebuttal (2025): In a randomized trial that finally measured hair as a clinical endpoint, 45 men took 5 g/day of creatine for three months. [2]
What they measured: hormone levels (testosterone, DHT) and hair changes (density, follicle count, hair thickness).
What they found: DHT barely changed, while hair density, follicle count, and thickness stayed flat.
⇥ The strongest studies to date point the same way: creatine does not cause hair loss.
Creatine and Coffee: Still Friends
🔴 Concern: The claim that caffeine “cancels out” creatine and perhaps shouldn’t be taken together traces back to an early study (Vandenberghe et al., 1996). Caffeine didn’t prevent creatine from entering muscle, but it appeared to blunt performance gains, possibly due to opposing effects on muscle relaxation time.
🟡 Rebuttal: Modern replication attempts (Trexler et al., 2016) failed to consistently reproduce this effect. So, the evidence never matured into something reliable or clinically meaningful. The only consistent issue seen in practice is that large doses of caffeine and creatine taken together can irritate the stomach.
🟢 Fix: If the combo irritates your stomach, split them up. Otherwise, carry on, and don’t overthink it. Coffee and creatine don’t need babysitting.
Your Next Move
Creatine makes lab reports a little noisier than most people know how to interpret but that doesn’t mean your kidneys should be concerned.
🎯 Troubleshoot The False Positives
In healthy individuals, creatine usage does not warrant routine monitoring of kidney function. The problem usually appears incidentally during annual labs or unrelated checkups, when creatinine levels are interpreted without context.
Creatine doesn’t fail people. Misread labs do.
Do not assess kidney function on creatinine alone. Let your physician know that you’re supplementing with creatine and ask them to use Cystatin C for routine labs.
This single adjustment prevents the most common downstream error: mistaking normal physiology for pathology.
Your Shift In Review
The comprehensive analysis of the literature delineates a safety profile for creatine monohydrate that is exceptionally robust.
The fear of kidney damage is unfounded in healthy individuals and is driven by a misunderstanding of serum creatinine kinetics. Long-term studies (up to 5 years) in athletes and clinical populations (ALS, Parkinson's) demonstrate preserved renal filtration.
The supposed creatine–baldness link was born from a single wobbly 2009 study. Fresh 2025 research that counted follicles one by one found no link between creatine and alopecia.
Creatine does not negatively impact blood pressure, hydration, or liver enzymes.
Avoiding creatine usually comes from reflex, not principle. Creatine moved from “maybe” to “of course” a long time ago. At some point, caution turns from seatbelt to handbrake.
Bodies that last are built by people who change their minds when the facts change. Tune up your judgement. Tune up your recovery. Rewrite the stories you inherited. It’s fine to hesitate. The mistake is never coming back to the question with better information. For the healthy adult, creatine monohydrate is a safe, well‑studied way to add muscle, speed recovery, and cognitive performance.
One Last Pulse Check
📁 Missed an issue? The archive is where the threads connect.
◀️ The prequel: Creatine's other job, the one your brain has been benefiting from.
🔍 Next issue: TBD. I have 12 ideas and zero certainty about which one wins, or when.
🏋🏽 Once a month I share my training logbook, what I'm testing, what I'm never doing again. I owe you one. The last three months have produced the worst resting heart rate and HRV numbers I've recorded since I started tracking. I'm developing three businesses, deep in software engineering, and debugging agentic loops at 1 AM. My body is currently drafting its own strongly worded resignation letter. Working on it.
📤 If you enjoyed this read, the best compliment I could receive would be if you shared it with one person who thinks creatine is just for gym rats.
I'm a Toronto doctor caring for older adults in hospitals and nursing homes, while spending my spare time digging into longevity science. I'm here to share what I'm learning. No fancy jargon, just practical insights to help you read your body’s early signals. Think of me as your friendly guide, figuring this out alongside you. Medicine has changed, but how we practice it hasn't caught up. That's why I'm here: to help you edit your health story while the early drafts are still open.
Appendix A
Study (Author, Year) | Duration | Dose Range | Outcomes Investigated |
Poortmans & Francaux (1999) 10 Healthy Athletes (n=9 + controls) | 10 months – 5 years | Spontaneous (1g – 80g/day) | The "Chronic" Benchmark: The first rigorous documentation of multi-year safety. Critical for refuting "cumulative damage" theories regarding glomerular permeability. |
Kreider et al. (2003) NCAA Football Players (n=98) | 21 Months | 15.75g/d (5 days) then 5-10g/d | The "High-Performance" Benchmark: Demonstrated safety under extreme physical/environmental stress. Debunked dehydration/cramping myths in contact sports. |
Groeneveld et al. (2005) ALS Patients (Age ~58) (n=175) | ~310 Days | 10g/day | The "Clinical" Benchmark: Applied a high dose (10g) to a vulnerable, older population. The large sample size (n=175) provides high statistical power for safety assertions. |
Bender et al. (2008) Parkinson’s Disease (Elderly) (n=60) | 2 Years | 20g/d (6 days) then 4g/d | The "Biomarker" Benchmark: Used Cystatin C to definitively prove that rising creatinine in users is a metabolic artifact, not renal failure. Essential for geriatric care. |
Neves / Chilibeck (2011/2015) Post-menopausal Women (n=~30-50) | 1-2 Years | ~3-5g/day | The "Female" Benchmark: Addressed the gender gap in safety data, confirming long-term tolerance in older women prone to osteopenia and sarcopenia. |
Appendix B
Systemic Concern | Scientific Reality | Key Findings | References |
Blood Pressure | Concern: Water retention increases blood volume and arterial pressure. Reality: Creatine may actually improve vascular health by reducing homocysteine and increasing nitric oxide bioavailability. | No Hypertension: Meta-analyses confirm creatine does not elevate blood pressure. Confounder: Adverse cardiac events (palpitations) are almost invariably caused by multi-ingredient pre-Workouts (high caffeine, stimulants), not creatine itself. | de Souza e Silva (2019) Mayhew et al. (2002) Cameron et al. (2018) Sanchez-Gonzalez (2011) |
Hydration | Concern: Creatine causes cramping and dehydration by "stealing" water from the body. Reality: Creatine is an osmolyte that drives water into the muscle cells. It does not deplete extracellular or vascular volume. | Protective Effect: Athletes on creatine report fewer muscle cramps, heat illnesses, and strains than placebo groups. | Kreider et al. (2003) Mayo Clinic (2023) Greenwood et al. (2003) |
Gastrointestinal Distress | Concern: Bloating, diarrhea, and stomach cramps. Reality: This is a genuine side effect. It is typically caused by undissolved crystals drawing water into the gut (similar to lactose intolerance). | Dose-Dependency: GI distress is linked to high bolus doses (e.g., >10g at once). Mitigation: Dissolving powder fully in warm water or splitting doses into 5g increments throughout the day eliminates this concern. | Groeneveld et al. (2005) Twycross-Lewis et al. (2016) |
Reply